

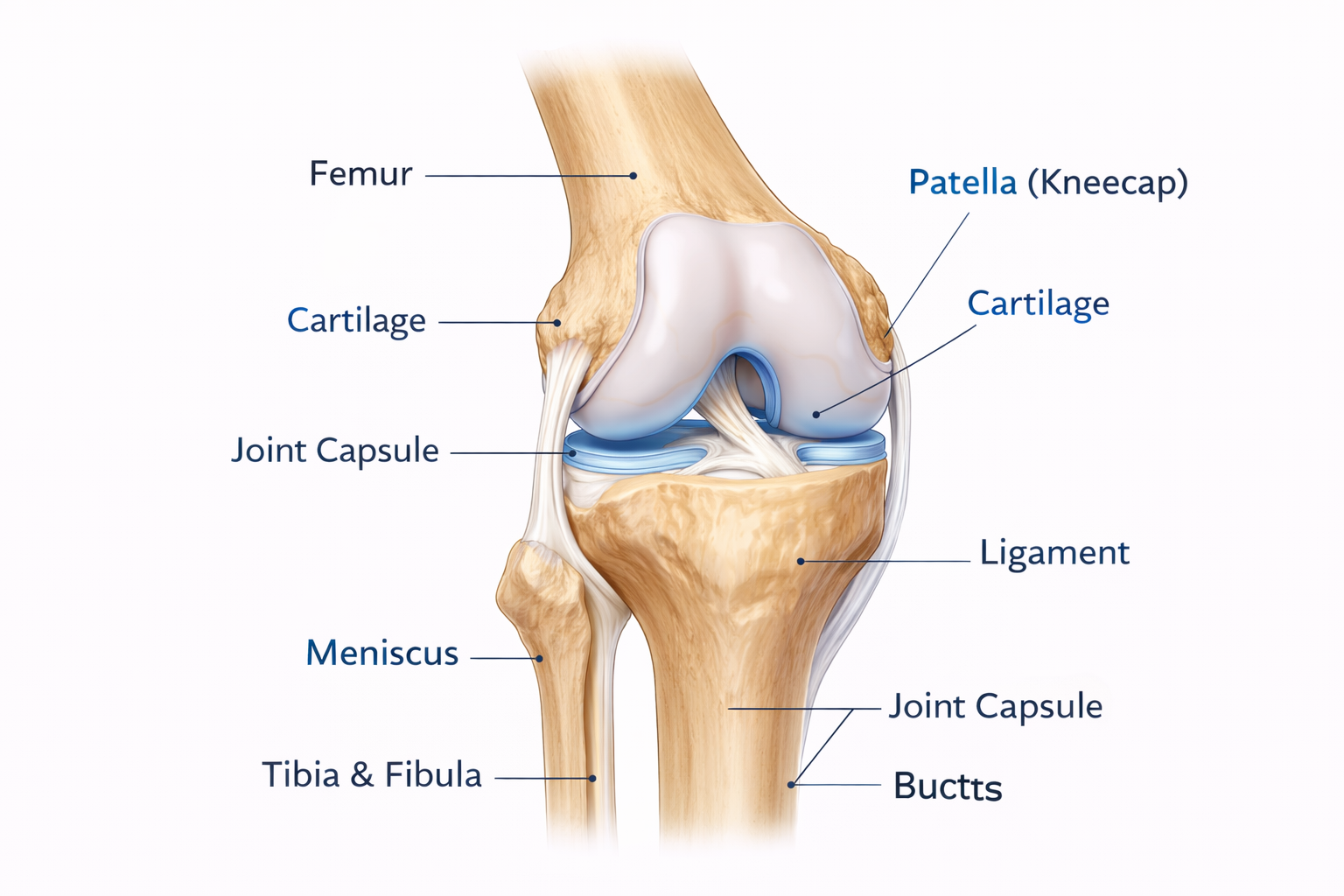

Total Knee Replacement (TKR)
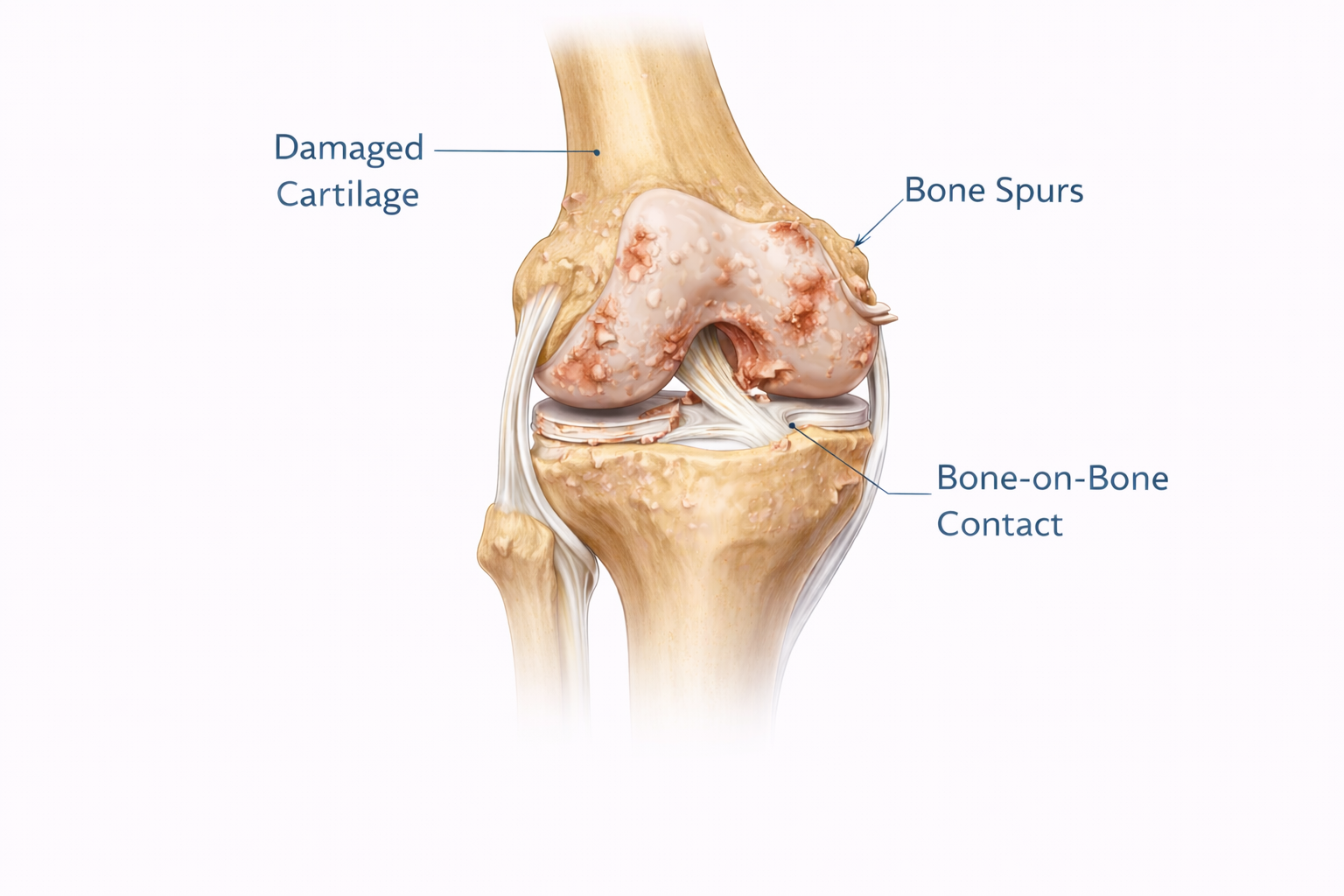
Removes damaged cartilage and bone from all three compartments (medial, lateral, patellofemoral) and replaces them with prosthetic components.
When it’s recommended
Severe arthritis across multiple compartments, significant pain & functional limitation, failed conservative care.
Pros
- Addresses all areas of joint damage
- High success rate (85–90% pain relief)
- Durable long-term outcomes
- Extensive research & proven track record
Cons
- Larger incision (8–10 inches)
- Longer recovery time
- More bone removal
- Higher revision risk if complications occur