Unsure about surgery? Get a trusted second opinion within 24-48 hours from the top orthopedic surgeons in the country.

Is It Actually Time for
Hip Replacement?
Finally — an honest look at the signs, the surgery options, and the recovery details you were never told about.
By the XPRT2ND Medical Review Team · 8 min read · Board-Certified Reviewed
500+
Hip replacements
performed annually in the u.s.
1 in 4
Adults over 60
Experience Chronic Hip Pain
85%
Patients report "excellent"
outcomes at 10 years
24-48h
time to recieve your
independent review
*Serving patients across Phoenix, Scottsdale, Tucson, and the greater Arizona area
Most people wait 7 to 10 years too long before addressing chronic hip degeneration. By the time they finally walk into a surgeon's office, the compensatory pain in their lower back and opposite knee has already taken hold. The question isn't just whether your hip is bad — it's whether the recommendation you received gives you the complete picture.
Total hip replacement (THR) and partial hip replacement are not just procedures for removing worn bone. They are decisions about reclaiming the ability to put on your own shoes without a strategy, get in and out of a car without wincing, and sleep through the night without a dull ache deep in your groin.
But like any surgery — especially a permanent, joint-altering one — the decision demands more than a 10-minute consult and an X-ray. In this guide, we'll walk through the five clinical signs surgeons use to recommend hip replacement, the distinctions most patients never hear about, and the one step that consistently replaces doubt with clarity.
1
SIGN ONE
Your Life — Not Just Your X-Ray
Surgeons look at scans. But you live in your body. The clinical threshold for hip replacement isn't a number on an imaging report — it's the point where your daily function has deteriorated enough that conservative care can no longer compensate.
The honest test isn't how bad your X-ray looks. It's how small your world has become. Three real-world scenarios that signal it may be time:
👟
The "Socks and Shoes" Test
Are you choosing footwear based on what you can get on without bending? Avoiding laces, low shoes, or anything that requires reaching your foot? That's functional limitation — not just discomfort.
🚗
The "Car Entry" Maneuver
Do you lift your leg with your hand to get into the driver's seat? Does getting in and out of a vehicle require a moment to plan? Hip flexion limitation at this level is a measurable clinical marker.
🪜
The "Staircase Stutter"
Is every step up or down a calculated risk? Do you lead with the same leg every time, or grip the rail to manage pain? Stair avoidance is one of the most reliable functional impairment indicators.
The Litmus Test: If you are planning your entire day around how many steps you take — mapping routes through buildings, choosing parking spots by distance, refusing social plans that involve walking — the hip is no longer just a joint. It has become a cage.
Not sure if your function loss is severe enough to justify surgery?
Have your imaging and history reviewed independently — by a specialist who has no stake in the outcome.
2
SIGN TWO
Total Hip vs. Partial Hip — What You Actually Need to Know
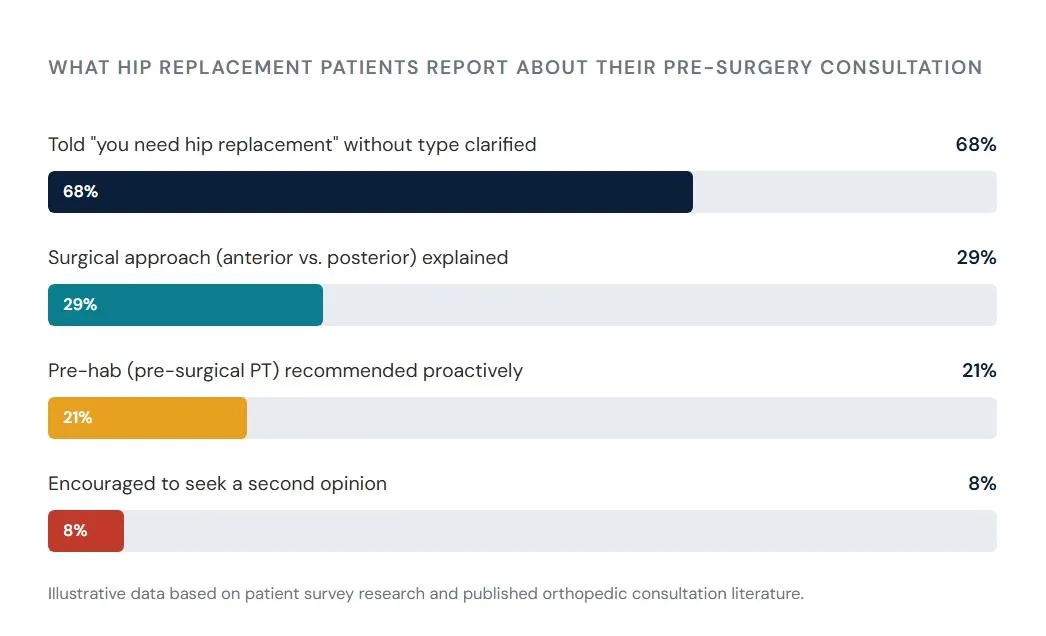
Most patients are told they need a hip replacement without fully understanding there are two fundamentally different procedures — and that the distinction matters enormously for recovery, long-term outcomes, and whether the recommendation matches your actual diagnosis.
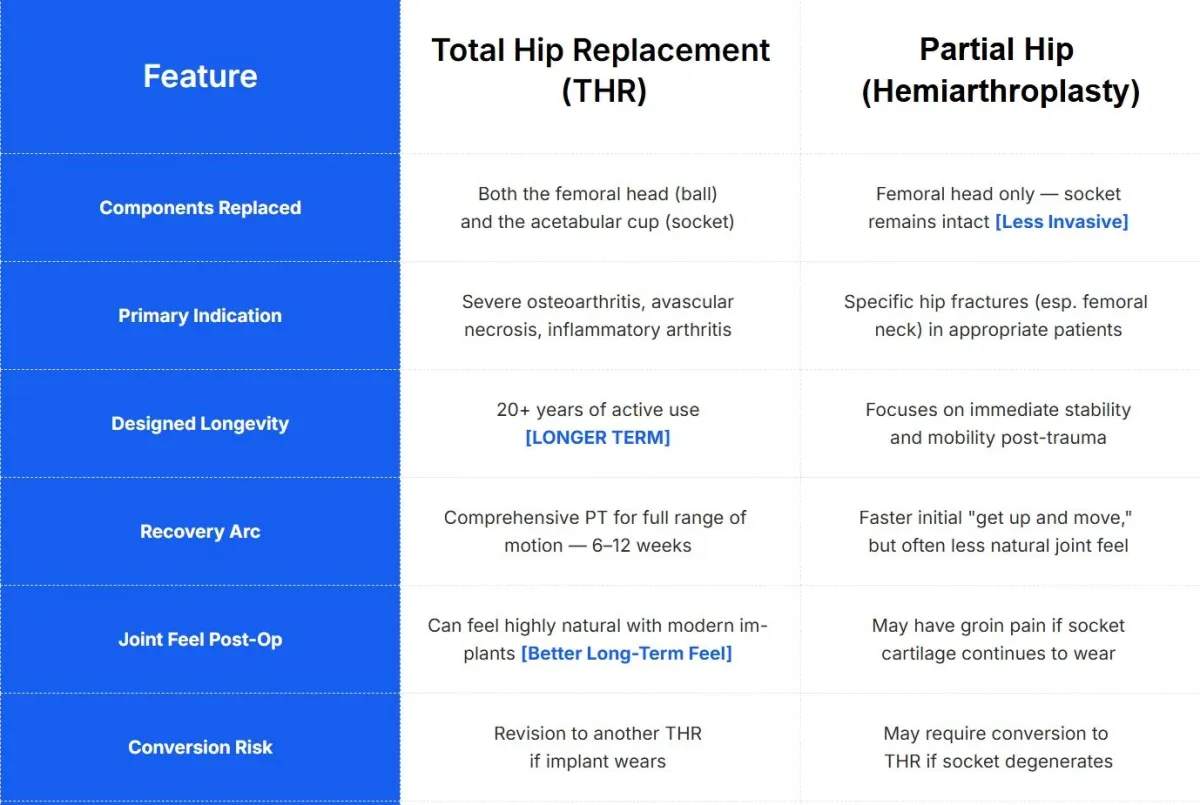
If you've been told you need a hip replacement but weren't clearly walked through which type and why your anatomy and diagnosis specifically points to that approach — that's a meaningful gap before you consent to anything permanent.
3
SIGN THREE
The "Groin" Trap — You're Probably Misidentifying Your Own Pain
One of the most common reasons patients delay getting the right diagnosis is that they're looking for pain in the wrong place. Hip pain has a famously deceptive anatomy — and many people spend years treating the wrong structure because no one explained this clearly.
True Hip
Joint Pain
— Is almost always felt in the groin or deep in the front of the thigh, not on the outside of the leg. If your groin aches when you walk or sit for long periods, that is the hip joint speaking.
The Common Mistake
— Pain on the outer side of the hip (the "hip" most people point to) is frequently bursitis or iliotibial band irritation — soft tissue issues that may not require surgery at all. These are often managed without replacement.
The Referred Pain Deception
— Pain on the outer side of the hip (the "hip" most people point to) is frequently bursitis or iliotibial band irritation — soft tissue issues that may not require surgery at all. These are often managed without replacement.
Lumbar Overlap
— Hip degeneration and lumbar spine pathology coexist and mimic each other. "Hip-Spine Syndrome" is a documented phenomenon where treating one without addressing the other leads to persistent symptoms post-surgery.
"If you've been treating "hip pain" conservatively for months without improvement, it's worth confirming whether the structure you're treating is actually the source — before committing to a surgical solution for the wrong problem."
XPRT2ND Medical Review Board
4
SIGN FOUR
The Robotic Surgery Question
Robotic-assisted hip replacement — platforms like Mako, ROSA, and Stryker's robotic arm systems — has become a significant marketing feature at large orthopedic centers. And the technology, used well, does offer genuine advantages in cup placement precision, leg-length accuracy, and reduction of dislocation risk.
But here is what the advertising doesn't say:
What Robotic Surgery Actually Means For You
The robot does not operate. It assists the surgeon in executing a pre-planned implant position — it is a guidance tool, not an autonomous system.
Cup angle and leg-length discrepancy — the two most common sources of post-op complications — are where robotic assistance offers measurable value. But only when programmed correctly by an experienced surgeon.
Surgeon case volume and institutional complication rates are still the most predictive factors in your outcome — more than the technology used.
In some facilities, robotic surgery is a premium pricing tier with modest additional clinical benefit for straightforward cases. In others, it is genuinely indicated by your anatomy.
The question to ask your surgeon isn't "do you use a robot?" — it's "why is the robotic approach specifically indicated for my anatomy and diagnosis, and what are your personal complication and dislocation rates?"
Was the conversation more about technology than your specific anatomy?
An independent specialist can review your surgical plan and tell you whether the approach is right for your case — not just your surgeon's preferred workflow.
5
SIGN FIVE
The Hidden Recovery Factor Nobody Mentions
Most resources talk about the surgery. Very few talk honestly about what determines whether your recovery is excellent or average. There are two factors that have an outsized impact — and most patients only learn about them after the fact.
The Anterior vs. Posterior Approach Decision
Anterior Approach (Front)
No "hip precautions" — fewer bending restrictions post-op
Faster initial recovery for many patient
Less disruption to the gluteal muscles
Risk of temporary lateral femoral nerve numbness
Technically demanding — best with high-volume anterior specialists
Posterior Approach (Back/Side)
More traditional, widely performed
Gives surgeon the best visualization for complex anatomy
Slight "no-bend" restriction period initially
Well-established long-term outcomes data
Often preferred for revision or difficult primary cases
Neither approach is universally superior. The right choice depends on your anatomy, your surgeon's volume and experience with each technique, and the complexity of your specific case. If no one explained why one approach was chosen for you — that's worth understanding before surgery.
The Muscle Atrophy Problem — The Secret to a 5-Star Recovery
Here is what almost no one says clearly: if you wait until you can barely walk to schedule surgery, your new hip will be mechanically sound — but the muscles around it will be too weak to drive it.
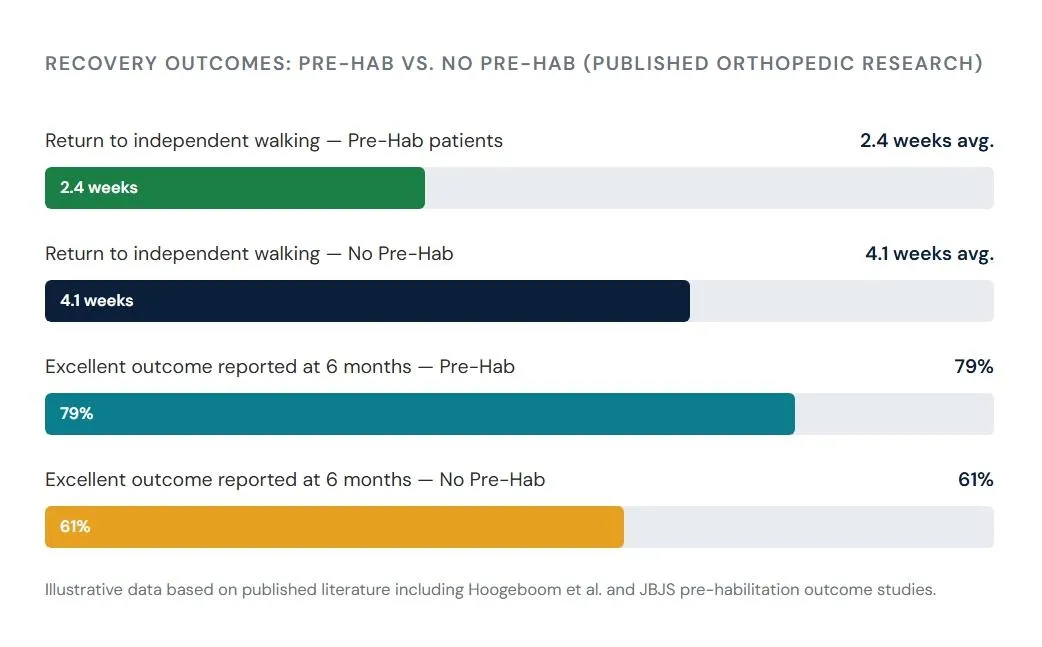
Pre-hab — structured physical therapy performed before surgery — is the single most underutilized predictor of post-surgical outcomes. Patients who undergo 4–8 weeks of pre-hab consistently show faster return to function, shorter hospital stays, and better outcomes at 6 and 12 months post-op.
Secure upload · Board-certified expert · Written review in 24–48 hours
Here's the Problem Nobody Says Out Loud
When you ask the surgeon who would perform your hip replacement whether you need the procedure — you are asking someone whose professional and financial interest is aligned with performing it.
That doesn't make them unethical. Most surgeons are excellent clinicians who genuinely believe surgery is the right path. But structural incentives exist, and informed patients — who've done their homework and sought independent confirmation — consistently report better experiences, better outcomes, and far less post-surgical regret.
Independent second opinions don't mean your surgeon is wrong. They mean you have a neutral, board-certified expert with no stake in your decision confirming the diagnosis, the timing, and the plan — before you commit.
"I'd been living with hip pain for three years before my surgeon said it was time. The consult was fast — maybe 8 minutes — and I walked out with a surgery date scheduled for six weeks later. My daughter found XPRT2ND and convinced me to submit my case. The specialist confirmed surgery was appropriate but noted I was a strong candidate for the anterior approach, which my original surgeon hadn't mentioned. That detail changed my recovery completely."
Diane K.
Age 64, Arizona · XPRT2ND Patient
Red Flags of a Rushed Recommendation
Not all orthopedic consults are equal. Pay close attention if you experienced any of the following:
The appointment lasted under 10-12 minutes before a surgical recommendation was made
Your most recent MRI was not reviewed — only an older X-ray
The surgical approach (anterior vs. posterior) was never discussed or explained
Risks including dislocation, leg-length discrepancy, nerve injury, or DVT were not covered in detail
Pre-surgical physical therapy (pre-hab) was not recommended or mentioned
You felt subtle pressure to schedule quickly to secure a date
Alternatives to total replacement — including partial hip or continued conservative care — were not explored
Your hesitation is not paranoia. It is instinct. And instinct before a permanent surgical decision deserves to be honored with information.
How XPRT2ND Works
We built XPRT2ND for exactly this moment — after you've received a surgical recommendation, before you've committed to the operating table.
Step 1 — Submit Your Case (15 minutes)
Upload your imaging (X-rays, MRI), your medical history, and the surgical recommendation you received. Our secure platform handles HIPAA-compliant file transfer.
Step 2 — Independent Expert Review
A board-certified orthopedic specialist — with no affiliation to your current provider and no financial stake in your decision — reviews your complete case history and imaging.
Step 3 — Written Clarity in 24–48 Hours
You receive a detailed written opinion: Is the surgery appropriate? Is the timing right? Is the recommended
approach correct for your anatomy? Are there alternatives worth pursuing first?
Step 4 — Walk Into Your Decision With Confidence
Whether the review confirms surgery or surfaces alternatives, you now have independent expert validation. The anxiety of uncertainty is replaced by the clarity of knowing.
Don't Walk Into Hip Surgery
With Unanswered Questions.
You already have the imaging. You already have the diagnosis. Now get a neutral, expert second set of eyes — with nothing to gain from your decision — to confirm you're making the right call, at the right time, with the right plan.
Secure
HIPAA-Compliant
Upload
Board-Certified
Orthopedic Expert
Written
Review in
24–48 Hours
No Surgical
Incentive. Ever.
No referral needed · Reviewed by a board-certified orthopedic specialist · Results in 24–48 hours
Our 48-Hour Review Guarantee
If you do not receive a thorough, professional written review within 48 hours of your case being accepted, we will refund your fee in full. No hoops. No games. We stand behind the process completely.
One Final Question
Hip replacement is the right decision for hundreds of thousands of people every year. The goal isn't to avoid surgery — it's to arrive at surgery with complete certainty that it's necessary, appropriately timed, and correctly planned.
Without Confirmation
Wondering if this was necessary
Unsure if other options existed
No neutral voice in the decision
Pre-hab opportunity potentially missed
With XPRT2ND Confirmation
Expert confirmed this is appropriate
All options were considered
Pre-hab strategy in place
Walking in with certainty
You can cancel a surgery date.
You cannot reverse a surgery that has already happened.
Secure upload · Board-certified expert · Written review in 24–48 hours
P.S. Most patients tell us the anxiety lifts immediately once they have a neutral expert confirm their decision. Whether the answer is "yes, proceed" or "here's what to consider first" — clarity is always better than doubt going into surgery.
P.P.S. If surgery is already scheduled, this is even more important. Confirming the approach, the timing, and the plan before the operating room is exactly what a second opinion is for.
P.P.P.S. Good surgeons welcome patients who've done their homework. If yours doesn't, that's important information too.
Clarity changes everything.
© Copyright 2026 xprt2nd.com-All rights reserved